
5.1. Start and Stop (Lead in/Lead out)
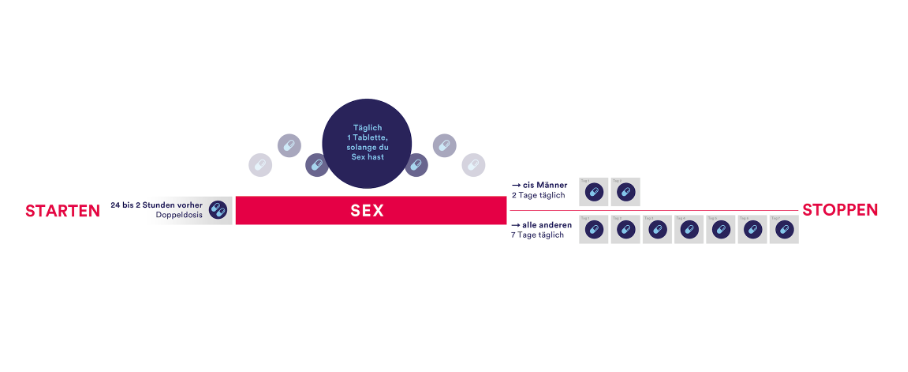
Whilst the first clinical trials used longer lead-in and lead-out phases of PrEP of 7 or even 28 days before and after a sexual risk, more evidence is available to support shorter lead-in lead-out phases. For cisgender men who have sex with men (MSM), a shorter lead-in and lead-out phase is feasible, as demonstrated by multiple studies following the IPERGAY protocol—also referred to as the “on-demand”, “event-driven” or “2-1-1” regime (5)(27). The IPERGAY study assessed PrEP with TDF/FTC given as two doses 2 to 24 hours before sex, one dose 24 hours after the first (double) dose, and one dose 24 hours later (‘2-1-1’ dosing). For consecutive sexual contacts, cisgender MSM were instructed to continue with one pill per day until two days after the last sexual encounter. With every new sexual encounter, PrEP was to be initiated with a double dose, unless the last PrEP dose had occurred within 7 days, in which case only one pre-exposure dose is recommended.
For cisgender women and other people who have receptive vaginal sex (including transgender men), longer lead-in and lead-out phase of 7 days due pharmacokinetic studies showing lower levels and a faster decay of tenofovir in the female genital tissue used to be recommended. However these studies actually show that protective levels of combined TDF/FTC were reached in 98% 2h after the oral intake of 2 pills of TDF/FTC (8). Regarding the optimal lead-out phase, the same study shows that the concentration was short-lived compared to colorectal tissue and therefore a 7 days lead-out phase should still be recommended to cisgender women and other people who have receptive vaginal sex. Many international guidelines therefore already include the new so called 2-7 regime for these populations. Although no clinical data exist on this regime so far, we still think evidence is good enough recommend this regimen for people who might otherwise choose no HIV protection at all. However, it is important that cisgender women and other people with receptive vaginal sex are made aware of this reduced level of evidence during the PrEP consultation.
Whilst there is a growing knowledge on the ideal start and stop time, some situations require special precautions:
Other regimens, such as continuous PrEP for four days a week (TTSS= Tuesday, Thursday, Saturday and Sunday) refer to retrospective data only and are therefore not recommended until further evidence is made available (studies still ongoing).
Figure 1: Lead-in/Lead out phases
5.2. Duration for PrEP intake
As the frequency of potential sexual exposure to HIV varies for each individual, different durations for the PrEP intake are used. Besides daily use, the most common regimen, some people with fewer sexual partners, prefer an event-driven regimen, where PrEP is only taken before and after a sexual contact.
An intermediate regime is the “Intermittent PrEP” or often called “holiday PrEP” where the PrEP is taken daily, but only over a limited period and with long intervals without PrEP.
8.1. PrEP start-up Syndrome
The PrEP start-up syndrome describes a variety of gastrointestinal and non-gastrointestinal symptoms that may occur in the first days and weeks of PrEP initiation. They are usually not associated with target organ damage, and are self-limiting after a few days until a maximum of 8 weeks (40).
Side effects can include nausea, flatulence, abdominal pain, dizziness, and headache. These symptoms occur early, but usually disappear within the first month. They can often be managed with a symptomatic treatment like analgesia or anti-emetics, if necessary.
8.2. Alterations in kidney function due to TDF and recommended surveillance
TDF is known to induce proximal renal tubulopathy (PRT), known as Fanconi syndrome, in some individuals (41). This is a very rare side effect where the proximal renal tubules do not absorb certain electrolytes and amino acids, resulting in a loss in the urine. Proteinuria, hypophosphatemia, hypokalemia, hypouricemia, renal acidosis and glucosuria, with normal blood glucose level, are characteristic of PRT as well as possible renal insufficiency and polyuria. In PRT, it is possible that despite the presence of proteinuria and hypophosphatemia, the creatinine clearance remains within the normal range. Most often, only some of these abnormalities are observed, and it is not certain which tests discriminate best for TDF renal toxicity.
8.2.1. Frequency of kidney function testing
After starting to take TDF for PrEP, a small but statistically significant decrease in creatinine clearance may be seen from baseline, which resolves after stopping TDF/FTC (42). There are no data for people with eGFR<60 mL/min, so continuing TDF/FTC if eGFR falls to below 60 mL/min/1.73 m2 is not advised.
Reduction in creatinine clearance while taking TDF/FTC alone is a rare side effect and many international guidelines now recommend checking the kidney function in healthy PrEP clients with no other risks for kidney failure only once or twice a year (43)(44). Although 6–12-monthly tests might be sufficient for people without risk factors, we recommend routine checking of kidney function at every visit for people considered at greater risk, for example, people with:
8.2.2. How to screen for kidney function
8.2.3. Stepwise approach in case of reduced GFR
In case of an alteration in kidney function, we recommend a stepwise approach (fig.3)
If a decrease in the GFR is confirmed, we recommend the following further investigations:
If laboratory tests confirm PRT, stop TDF/FTC and test kidney function again after 4 weeks. A change from a TDF to a TAF-based PrEP regimen can be considered (29). However, TAF is not currently authorized by Swissmedic for prevention in Switzerland, and there are no generic versions available in Swiss pharmacies. Formally, the FDA label is only for people with a GFR >60 mL/min.
If lab results do not confirm PRT, still consider stopping PrEP, especially if GFR is <60 and refer the client to a kidney specialist.
Figure 3: Stepwise approach in case of alteration in kidney function
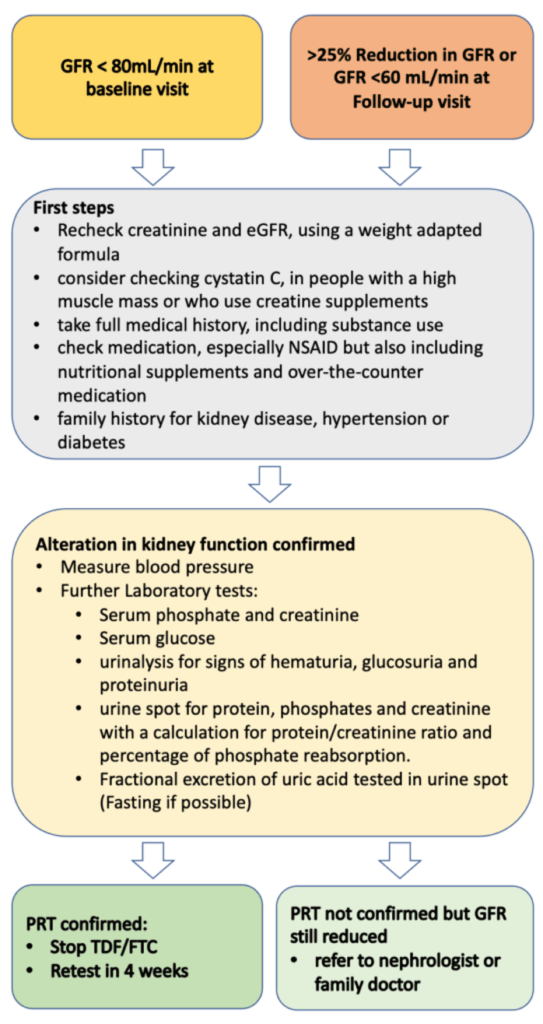
GFR= Glomerular filtration rate, NSAID= nonsteroidal anti-inflammatory drug, PRT= proximal renal tubulopathy, TDF= Tenofovir disoproxil fumarate, FTC= Emtricitabine
8.3. Increase in levels of liver enzymes
TDF can cause a mild to moderate increases in liver alanine aminotransferase (ALT) in some people living with HIV (45) and in some PrEP users (46). The clinical relevance of these findings is unclear, and most guidelines do not recommend including ALT tests in regular PrEP visits (43)(44). To our current knowledge, cases of severe PrEP induced liver injury have not been reported. As mild elevation of liver enzymes is common in the general population (prevalence estimates mostly >10%) (47), elevation of liver enzymes in PrEP clients is likely to have other origins than TDF induced liver toxicity, e.g. alcoholic liver disease (ALD), non-alcoholic steatohepatitis (NASH). Liver toxicity due to recreational drug use and viral hepatitis might be more common in PrEP clients than in the general population.
The benefits (early detection of disease and potential drug toxicity) and risks (overdiagnosis, stopping PrEP unnecessarily, complications of further examinations, costs) of screening in PrEP clients are unclear, and evidence informing a recommendation is lacking. Furthermore, the upper limit of normal (ULN) for transaminases is disputed. Values in the normal range do not exclude liver diseases (48), and subsequent diagnostic evaluation of mildly elevated transaminases often do not find specific liver diseases (34). By taking into consideration that PrEP is prescribed to healthy clients as prevention, we recommend testing for ALT before starting PrEP, at the safety visit and every 12 months thereafter, until more data on liver toxicity is available.
If elevated liver enzymes are observed, other reasons than PrEP intake should be considered. For non-acute and asymptomatic patients, we propose a stepwise approach detailed in the algorithm below (fig.4), which we developed in adaptation to the EACS guidelines (3). When a persistent or significant ALT-elevation (>2x ULN) is observed, a basic assessment of the most common liver pathologies should be conducted. In the basic assessment, toxicity due to other medication and substances (e.g., anabolic steroids, cocaine, ecstasy), ALD, NASH, hemochromatosis, viral hepatitis and symptoms indicative of systemic diseases involving the liver should be evaluated. Individuals should be evaluated for liver steatosis with ultrasound and, if present, a fibrosis risk assessment using an established score conducted (e.g., Fib-4) (48). A low-risk score allows for periodical reassessment. For moderate results preforming transient elastography and for high-risk scores, a hepatologist referral is recommended (3)(48). If available, a transient elastography might be considered in the basic evaluation, but in most guidelines, ultrasound is recommended as the primary first screening tool for NAFLD (3)(48)(49)
If no cause can be identified, and the elevation of liver enzymes persists, rare causes (autoimmune liver and metabolic liver diseases) should be evaluated. Furthermore, stopping PrEP and a hepatologist referral should be considered. For significantly elevated liver enzymes (≥ 5.0 x ULN), acute onset and/or symptomatic patients, the proposed algorithm should be used with caution and a timely, comprehensive evaluation and hepatologic referral should be evaluated. It is important to emphasize that the finding of liver steatosis might have multiple origins. If, despite lifestyle interventions, the ALT-elevation progresses or fibrosis develops, other causes should be considered.
Figure 4: Stepwise approach for elevated ALT
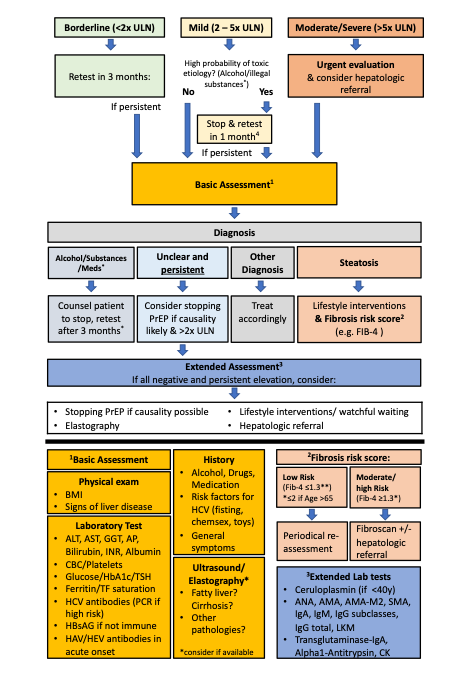
4 Alcohol and substance use leading to elevated liver enzymes is often caused by a problematic use or addiction which cannot be easily stopped. Counsel to stop and retest after 1 month is often insufficient in such situations. Consider referral to addiction medicine
ULN=Upper Limit of Normal, PrEP=Pre-Exposure Prophylaxis, BMI=Body-Mass-Index, ALAT=Alanin-Aminotransferase, ASAT=Aspartate-Aminotransferase, GGT=Gamma-Glutamyl Transferase AP=Alkaline Phosphatase, INR= International Normalized Ratio, CBC=Complete Blood Count, HbA1c= Glycated Hemoglobin, TSH=Thyroid Stimulating Hormone, TF=Transferrin, HCV= Hepatitis C Virus, HbsAG= Hepatitis B Antigen S HAV= Hepatitis A Virus, HEV= Hepatitis E Virus IgA Immunoglobulin A, IgM= Immunoglobulin M, IgG= Immunoglobulin G, LKM= Anti–Liver-Kidney Microsomal Antibody, CK= Creatine Kinase
8.4. Decrease in bone mineral density (BMD)
The use of TDF in people living with HIV is associated with an early decrease of 3-4% of bone mineral density after treatment start, especially when co-administered with a boosted protease inhibitor (50). In HIV-uninfected individuals using TDF/FTC as PrEP, this effect seems to be less pronounced (~1%) without increased fracture risk (42)(51)(51)(52). No routine screening with bone densitometry is necessary for individuals using PrEP. Increased physical activity, smoking cessation, and reduction in alcohol consumption may reduce the long-term fracture risk in all individuals, and calcium supplementation may be considered if intake is insufficient. The ten-year fracture risk should be assessed in individuals with risk factors for osteoporosis (e.g., history of falls or fracture, use of glucocorticoids) using the FRAX score, and bone densitometry should be performed in those with a high fracture risk to further assess the need for treatment. As the clinical consequences of the bone density reductions associated with PrEP remain unclear, the decision if TDF/FTC based PrEP should be prescribed in the presence of osteoporosis depends on the individual’s risk for HIV infection. For person’s with less sexual risks, switching from a daily to an event-driven regime to reduce TDF exposure might be beneficial to reduce the risk of a further reduction in bone density.